Plasma Biomarkers Show No Significant Link to Myasthenia Gravis Severity in New Study
Plasma concentrations of neurofilament light chain (NfL) and glial fibrillary acidic protein (GFAP) do not differ between patients with myasthenia gravis (MG) and healthy controls, according to a study published via PubMed. The research found that neither biomarker correlated with the Myasthenia Gravis Activities of Daily Living (MG-ADL) scale or the Myasthenia Gravis Composite (MGC) score, suggesting these specific proteins may not serve as reliable indicators of disease activity or severity in MG patients.
How do NfL and GFAP function as biomarkers?
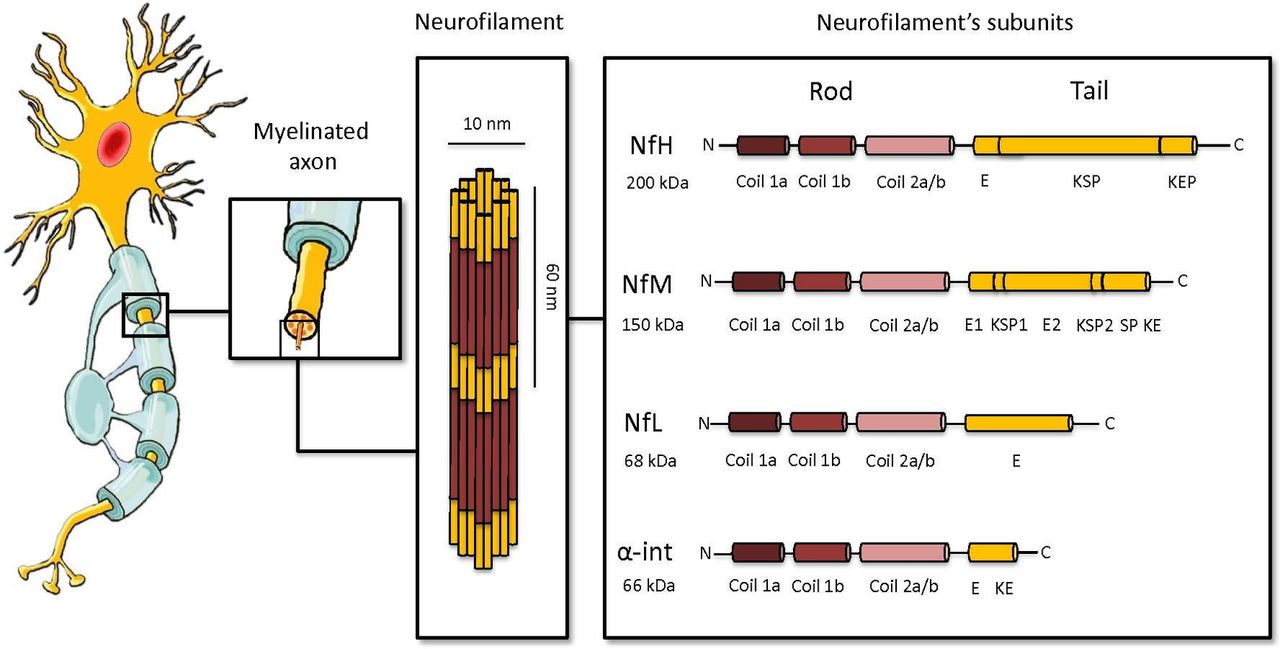
Neurofilament light chain (NfL) is a protein found in the axons of neurons. When neurons are damaged, NfL leaks into the cerebrospinal fluid and eventually the blood. Glial fibrillary acidic protein (GFAP) is primarily found in astrocytes, the support cells of the central nervous system, and typically increases during astrocyte activation or injury. Both are frequently used in neurology to track neurodegeneration or acute brain injuries.
In the context of myasthenia gravis—a chronic autoimmune neuromuscular disease that causes weakness in skeletal muscles—researchers tested whether these markers could signal systemic nerve or glial damage. However, the study results indicated that plasma levels of these proteins remained stable regardless of the patient’s MG status or the severity of their symptoms.
Why did the biomarkers fail to correlate with MG-ADL and MGC?
The lack of correlation with the MG-ADL and MGC scores is significant because these tools are the primary methods clinicians use to measure a patient’s functional impairment. The MG-ADL focuses on the impact of the disease on daily activities, while the MGC provides a more comprehensive assessment of muscle weakness.
Because MG is primarily a disorder of the neuromuscular junction—where the nerve meets the muscle—rather than a primary disease of the axons or the central nervous system’s glial cells, the researchers found no statistical difference (p > 0.05) between the MG group and the control group. This suggests that the pathology of MG does not trigger the same type of axonal or astrocytic leakage seen in conditions like multiple sclerosis or traumatic brain injury.
What are the implications for MG diagnosis and monitoring?
The findings suggest that NfL and GFAP are not effective tools for monitoring the progression of myasthenia gravis or assessing the efficacy of treatments. For athletes or high-performance individuals dealing with autoimmune conditions, the search for a “blood test” that can quantify daily muscle fatigue or recovery remains focused on other markers, such as acetylcholine receptor antibodies.
Medical professionals typically rely on electromyography (EMG) and antibody testing for definitive diagnosis. This study reinforces that systemic markers of general neuronal damage do not necessarily reflect the specific dysfunction occurring at the neuromuscular junction in MG patients.
How does this compare to other neurological markers?
While NfL is a highly sensitive marker for diseases like Amyotrophic Lateral Sclerosis (ALS) or certain types of dementia, its utility is limited in MG. In ALS, the degeneration of motor neurons causes a massive release of NfL into the plasma. In contrast, MG involves a blockade of receptors at the end of the nerve, leaving the axon itself largely intact. This explains why the plasma concentrations in the PubMed-cited study did not differ between the MG cohort and the healthy controls.

For those tracking these developments, the next step in neuromuscular research involves the identification of more specific biomarkers that can predict “crisis” events or response to new biologic therapies. Official updates from neurological societies and peer-reviewed journals will provide further clarity on emerging diagnostic tools.
Do you have experience with neuromuscular monitoring or follow these medical advancements? Share your thoughts in the comments below.

